
Recovery techniques - What you need to know - Part 1
By Kurt Jepson
 This concept is well established, having been developed in the 19th century, primarily via the work of Russian physiologists, including Ivan Pavlov (Viro A, J Appl Physiol, (92) ;2002).
This concept is well established, having been developed in the 19th century, primarily via the work of Russian physiologists, including Ivan Pavlov (Viro A, J Appl Physiol, (92) ;2002).
 The concentration of “lactic acid” is not the cause of muscular “soreness”, (Schwane JA, et al. Phys Sportsmed. 1983, 11(3)), but rather the result of fiber “microtrauma “, and the related soft tissue inflammatory mediators precipitated by the stress of the activity. Lactate acid does not linger in the interstitial region of the muscle, but instead quickly migrates into the blood stream for processing. It`s role regarding intramuscular “delayed” onset muscle soreness (DOMS), is absent.
The concentration of “lactic acid” is not the cause of muscular “soreness”, (Schwane JA, et al. Phys Sportsmed. 1983, 11(3)), but rather the result of fiber “microtrauma “, and the related soft tissue inflammatory mediators precipitated by the stress of the activity. Lactate acid does not linger in the interstitial region of the muscle, but instead quickly migrates into the blood stream for processing. It`s role regarding intramuscular “delayed” onset muscle soreness (DOMS), is absent.




High volume trainign season is under way and having a sound strategy for recovery from long or hard efforts in training or competition is vital to success. As the season progresses and the accumulated load builds, consistent implementation of recovery techniques becomes exponentially important.
Most athletes currently employ various tasks for recovery which they have adopted over the years, and anecdotally “work for them.”
RECOVERY BASICS
The metabolic cost of vigorous cross-country skiing is extremely high. Energy systems and muscles are recruited based on “need not speed”, thus anaerobic and aerobic pathways are continuously utilized by the body.
The musculoskeletal skill set required for high intensity efforts includes; dynamic agility, eccentric load dispersion, explosive concentric movements, stabilizing co-contractions, vibration dampening and extensive time spent in a state of “physiologic debt.” Cumulatively, this results in metabolites which inhibit the body’s ability to” Super-compensate” and elevate future performance.
One metabolite frequently monitored in athletes is Lactate (La). It`s blood concentration level is commonly used as an indirect indicator of fitness (Goodwin et al. J Diabetes Sci Technol. 2007; 1(4)). Resting levels are typically in the 1-2 mmol/L and can rise to ~20mmol/L with intense exercise (https://health.ucdavis.edu/sports-medicine/resources/lactate).
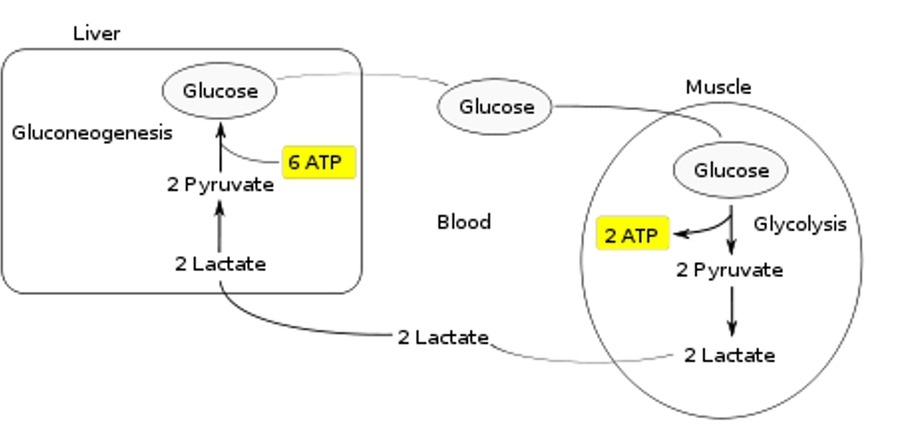
Simplistically, this compound is the byproduct of intense exercise which necessitates glycolysis as the cellular energy pathway. When glycogen is broken down in the absence of sufficient oxygen, such as during vigorous efforts where respiratory function can not keep up with muscular demand, lactic acid is produced.
In a well-trained individual, lactic acid is quickly disassociated into lactate molecules and hydrogen (H+) ions. The H+ ions are expelled via respiration and the lactate travels via the bloodstream to the liver for conversion back to glucose. When exercise demands via sustained intensity and/or duration exceed the ability of lactate “re-cycling”, acidosis results, pH is altered, and cellular function is subsequently affected. The result is fatigue and power production compromise.
Skiing is tough on a body. Dehydration, pH imbalance, enzyme alteration, structural damage, Cortisol (stress hormone) secretion and even psychological fatigue must all be addressed via recovery.
The connection between physiologic and psychologic stress cannot be overlooked. A 1995 study by Perna and McDowell (Int J Behavioral Med) looked at the exhaustive exercise response and subsequent recovery timeframe, in two groups of elite endurance athletes. They found Cortisol concentrations in the “high stress (psychological)” cohort persisted up to 20 hours longer than that identified in the “low stress” group.
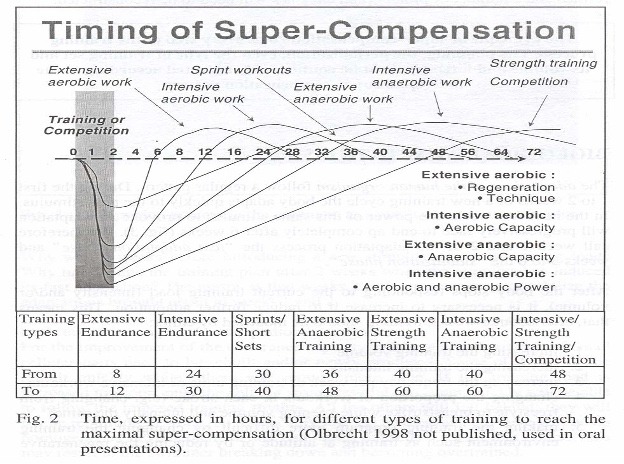
The extent of recovery participation should also be specific to the precipitating work load. The more “intense” the workout, the more time is required to adequately recover, as the chart depicts below.
Homeostatic normalization and regeneration levels for; muscle, bone, energy systems, neurokinetic pathways, blood volume, etc. occur at different intervals. This is an important concept for the athlete to remember when planning training activities.
For example, a 4 rep per set “max lift” session in the gym may necessitate a greater allotment of recovery time, than even a vigorous plyo workout.
This article will summarize the scientific efficacy of various strategies for recovery. This list is not fully inclusive, but addresses a few of the strategies commonly utilized.
MASSAGE
Let’s get this one out of the way first. Massage does not “clear” Lactate. Byproducts of energy production (via the Kreb`s Cycle) and muscle contraction, do not persist in the muscle tissue itself, but rather are released into the blood stream instantaneously. These substances must then be metabolized/converted by the heart, liver (gluconeogenesis), kidneys, etc. The time frame required for this is not directly influenced by massage. Most lactate is managed by the body within the first hour following exercise cessation.
If massage had a beneficial input to circulatory exchange and oxygen delivery, then in theory, it might assist in the normalization of the muscle unit in terms of its biochemical environment. The presence of free hydrogen ions, increased phosphocreatine, and elevated carbon dioxide concentrations, all have the potential to delay the resolution of “damage” caused by vigorous fiber contraction.
Unfortunately, there is no scientific evidence to indicate massage affects intra-muscular blood flow.
Many studies examining the effects of massage run into validity issues. Difficulties related to the “objective” (i.e. dose, technique, replication) delivery of the manual tissue stimulus to numerous subjects, small monogenous sample groups, subjective pain scale utilization, and measurement of macro- and microvascular blood flow, all taint reliability. Utilization of doppler ultrasound has assisted with blood flow monitoring, but the other parameters remain a challenge for any investigator.
In 1997, Peter Tiidus, PhD did an exhaustive literature review on post exercise massage and its relationship to muscle recovery (Manual Massage and Recovery of Muscle Function Following Exercise: A Literature Review. JOSPT, Vol 25 (2), 1997). His findings indicated there was little scientific data to support the practice of post exercise massage if the intent is to; address muscle fiber damage following eccentric exercise, retain muscle strength and performance, or address delayed onset muscle soreness (DMOS) induced by exercise.
Of course, the response to the above reference is, “yeah, but that study is now 25+ years old!” A valid concern. However, recent literature has not provided addition information which would contradict Tiidus`s conclusions.
H. Davis and S. Alabed et al published a large meta-analysis (n=29 studies) in 2020 (BMJ Open Sport and Exercise Medicine, 2020, 6) entitled; “Effect of sports massage on performance and recovery: A systematic review and meta-analysis.” They found that massage provides no significant improvement in measures of performance (i.e. jump, sprint, strength, endurance, fatigue). It seems to have a small but significant effect on flexibility when compared to no intervention, such as stretching. It also seems to have a small but significant effect on reducing DOMS. They concluded, as did Tiidus 20+ years earlier; “Our study finds no evidence that sports massage improves performance directly, it may “somewhat” improve flexibility and DOMS.”
In 2018 Zagozdon, LMT, reviewed hundreds of “studies” which included the term “massage” and found little scientific evidence that massage could influence muscular circulation, accelerate the processing of “toxins”, or enhance strength. M. Brown PhD, LMT concluded the same in 2022. Both practitioners are respected American Massage Therapy Association (AMTA) educators.
There are a few publications that support massage as a means of enhancing the flexibility of a muscular region via the short-term influence on the mechanical modulus of the fibers, and the surrounding fascia. Crommert et al in the Scandinavian Journal of Medicine and Science in Sports, vol 25 (5), 2014, noted an immediate but short-lasting reduction in muscle stiffness following a 7-minute protocol of massage on the medial gastrocnemius/calf muscle of 18 young men. They found that shear elastic modulus, their measure of flexibility, returned to baseline levels after just 3 minutes post massage.
Medeiros et al investigated the efficacy of using a foam roller as a recovery tool post exercise (The Effects of One Session of Roller Massage on Recovery from Exercise-Induced Muscle Damage: A Randomized Controlled Study, J Exer Sci and Fitness, 18, 2020). Thirty-six young men (n=36) completed exhaustive forearm isokinetic exercise movements. Baseline and post foam use data was collected on; range of motion (ROM), maximal volitional contraction (MVC) and delayed soreness (DOMS). They concluded that a single session of foam rolling had no effect on the recovery of the muscles tested. They did not comment on the more consistent use of a roller.
Manual therapy likely provides “superficial” sympathetic stimulation for vasodilation, and perhaps the lymphatic system. This response may assist in extracellular fluid exchange within the “superficial” myofascial layers, thereby enhancing cellular structural repair and normalization at that level only. Muscle functional performance is likely unaffected.
The take away from the concept of utilizing massage as a recovery modality is simple. If you can afford and have access to it, it likely does no harm. That said, if provided in a vigorous manner post exercise, it has been linked to creatine kinase release and Rhabdomyolysis, a metabolic process related to muscle fiber damage typically via a crush injury. Aggressive techniques should be avoided. The same goes for foam rolling.
Massage should not be considered a viable recovery modality if the athlete`s goals include lactate clearing or muscle performance enhancement.
The psychological aspect of massage, is a topic for another discussion.
Coming up in part two: what are viable forms of recovery? We look at
MECHANIZED PERCUSSIVE RECOVERY TOOLS , COOLING , CONTRAST AND THERMAL TREATMENT , ELECTRICAL STIMULATION , INTERMITTENT PNEUMATIC COMPRESSION , and
ACTIVE RECOVERY.