
Hip Flexors and athletic postuRing
By Kurt Jepson







Skiers use a variety of training modalities that will impact muscles and tendons around the hips. Classic skiing, running, skate skiing, even double poling can cause tightness that can affect hip faction and positioning.
Adding “targeted” flexibility exercise into our weekly sessions fits nicely in the spring. I use the term “targeted” because athletes typically have isolated musculoskeletal imbalances which affect efficient postures and limb function. This is particularly true after a long competitive season where the body has been generating forceful, repetitive, contractions to develop velocity. Adaptive shortening of some muscle groups and conversely, functional elongation of others, often lends to single or multiplanar positional shifts across joints which effect balance, power production and perhaps injury predisposition.
Thorough flexibility sessions to address acquired restrictions during the comp season usually take a back seat to nutrition, sleep, foam rolling, equipment management, travel, etc. Now is the perfect time to include targeted stretching into your week.
It should be mentioned here that “static” stretching is undertaken with the goal of correcting a postural imbalance or enhancing movement efficiency, not direct injury prevention. There is minimal literature that correlates static stretching to muscle injury prevention and conflicting studies whether static stretching may actually predispose one to injury. McHugh and Cosgrave authored and excellent retrospective review of the topic in 2010 (Scand J Med Sci Sports. 2010;20: 169-181). One could make the case that employing static stretching into a dynamic warm up routine, as a component to address any musculoskeletal imbalances, indirectly lowers “overuse” (not acute) injury risk.
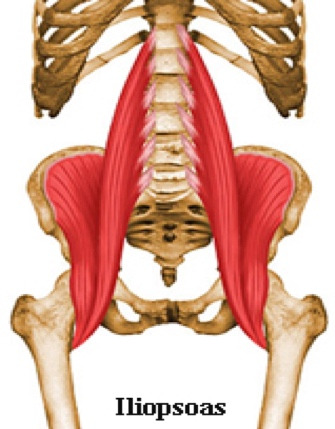
A frequent imbalance seen in cross country skiers involves the hip flexors. Restrictions in the Iliopsoas (IP) and Rectus Femoris (RF) groups develop due to habitual flexion postures of the core and lower extremity required to ski powerfully. Biomechanical cues such as; relaxed shoulders, knee and ankle flexion, dynamic compression, etc. all contribute to anterior postural dominance of our hips and core. The IP and RF muscle groups cross the lumbosacral and hip regions. Both have powerful inputs to trunk and hip flexion as well as secondary rotational actions on the hemi-pelvis and Femur. Unlike many muscles, the IP maintains its ability to produce extensive contractile force, regardless of its angular relationship to those skeletal components it is acting on. This is due to a unique origin and insertion which allows the IP to maintain parallel fibers and maximal tension via fibril overlap. Most muscles loose power as they become long, short or pull at an obtuse angle.
Due to the above characteristics, the Iliopsoas is an efficient compensator for weak abdominals and hip rotators vital to skiing. As such it is frequently overtaxed. When tight, the IP and the RF also have the ability to influence pelvic/core position away from stable neutral postures. Past Nordic Solution articles on core and hip conditioning have discussed this topic in depth.
Hip flexor anatomy: Anterior dominant skiing posture:
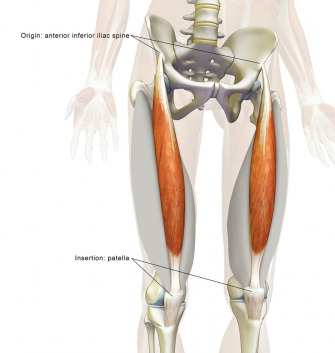
Rectus Femoris anatomy:
Restrictions anteriorly in the Psoas and Rectus Femoris groups have been associated with adverse pelvic and core postures for years. The concept of a “dumped pelvis” resultant of “lower crossed syndrome” was described by Czech physician Vladimir Janda in 1979. He proposed that with Psoas and Rectus Femoris tightness, the anterior aspect of the pelvis would be tilted inferiorly (downward) resulting in chronic shortening and weakness of the hip flexors. Concurrently the frontal pelvic rotation would increase lumbar lordosis, adding to compression load there. Additionally, the gluteal musculature would experience “stretch weakness” as described by Kendall, Kraus, Brugger and others.
Dumped Pelvis and resultant impairments:
Potential sequalae from the above functional position can include;
- Compression injury to the posterior elements of the lumbar spine such as the disc wall, facet joints, interspinous ligaments, and vertebral stress fractures (i.e. Pars Interarticularis)
- Sacral Iliac Joint issues
- Avulsion injury, and in the adolescent athlete apophysitis, of the origin of the Rectus Femoris
- Femoral Acetabular Impingement syndromes and early degeneration
- Hip flexor and Adductor strains
- Snapping Psoas Syndrome
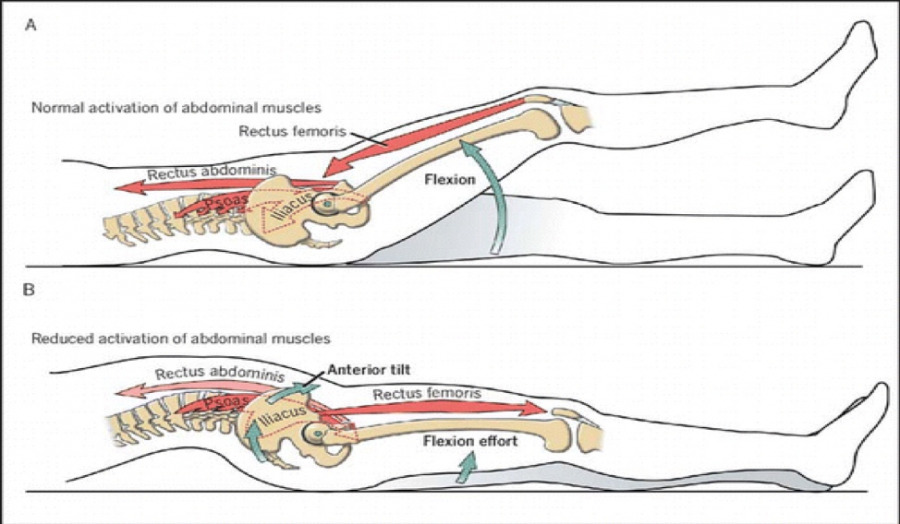
Physical Therapists spend significant time with their hip and low back patients describing the perils of excessive Anterior Pelvic Tilt and devise exercise programs to negate the malady. “Static” stretching of the quadriceps, psoas, and lumbar paraspinals (if needed) with concurrent activation and strengthening of the abdominal, gluteal and hamstring musculature are the mainstay of most treatment plans. Special care is taken to focus on neutral core positions and to avoid abdominal exercises that inadvertently recruit the Iliopsoas as a trunk flexor. It has been well established that anterior dominant postures and excessive IP activity during hip and core exercise places dramatic compressive and shearing loads on the lumbar spine.
Many classic hip abductor and core activation exercises have high levels of IP recruitment which may be disadvantageous to the athlete if isolated work is the goal, or there is an injury to the IP/RF.
Examples with potentially unwanted side effects include; Clamshell external rotation movements, bilateral supine leg raise activities and side lying hip abductor exercises. All of these activities produce EMG activity of ~ 30-45% in the IP which indicates sufficient neuromuscular recruitment for irritable contractile load (Philippon M, et al, Rehabilitation Exercise Progression for the Gluteus Medius with Consideration for Iliopsoas Tendinitis. An In Vivo EMG Study. Amer J Sports Med.2011, 39(8), 1777-1785).
The key to avoiding unwanted hip flexor imbalance is compliance with a targeted flexibility and abdominal activation program. Simply put, the IP, RF and Tensor Fasciae Lata / ITB (also a strong flexor when the hip is in relative extension) must gain length/flexibility and the layers of the abdominal wall strengthen/tone, particularly the Rectus Abdominus (RA).
Doing so negates Anterior Pelvic Tilt and better positions the core and pelvis for athletic movements as depicted below.
When we think of “core activation” while performing an athletic movement, we are effectively positioning our pelvis away from a “dumped” posture and encouraging Posterior Pelvic Tilt to neutral. The Transverse Abdominis (TA), RA and Obliques all participate in this endeavor.
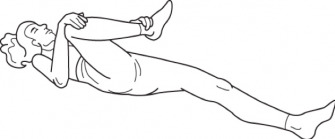
Exercises to address the postural imbalance described are familiar to most fitness enthusiasts. A few examples include;
Quadriceps stretching in sidelying.
Combined low back and hip flexor stretch off an elevated surface.
Hip rotator stretching.
Rectus Abdominis and Oblique strength exercises with minimal Iliopsoas contribution (including EMG %`s). Anything less than 30-40% MVC is acceptable. (Quantitative Intramuscular Myoelectric Activity of Lumbar Portions of Psoas and the Abdominal Wall During a Wide Varity of Tasks. Juker D, McGill S, et al. Med Sci Sports Exer. Feb (30), 1998
Side Bridge, knees flexed (12-21%).
Range limited crunch (7-18%),…….vs full sit up variations 35%+
Squat with up to a 100kg load (5-16%).
In athletics we must always consider the relative “cost” of those training activities we engage in. Unfortunately, many of the exercises we select to improve our hip and core strength and the act of skiing itself, place us at risk of postural imbalance and injury. The hip flexors are one such area. Athletes need to place special emphasis on flexibility and lumbopelvic balance during the off season, and continue that work periodically throughout the year.