
Physiological effects of altitude - PaRt 1
By Sarah Willis, PhD
 When we travel to higher elevation (altitude) for a race, on-snow camp, or residing at altitude, there are physiological effects on our body regarding how it responds and adapts to this environment. The feelings of these effects are most intense at the start when first arriving at a higher altitude. For certain individuals, it is possible to have feelings already at 2,000 ft including symptoms of lightheadedness, higher heart rate, gastric distress, dehydration, and decreased performance (Bärtsch and Saltin, 2008).
When we travel to higher elevation (altitude) for a race, on-snow camp, or residing at altitude, there are physiological effects on our body regarding how it responds and adapts to this environment. The feelings of these effects are most intense at the start when first arriving at a higher altitude. For certain individuals, it is possible to have feelings already at 2,000 ft including symptoms of lightheadedness, higher heart rate, gastric distress, dehydration, and decreased performance (Bärtsch and Saltin, 2008).
As far as training and exercise goes, SLOW DOWN and adjust your pacing strategies. This is especially important in the first 3-4 days upon arrival, maybe longer. It can be very helpful in this environment to use morning heart rate as a recovery monitoring tool (see Training Periodization : Monitoring Recovery posted on Nov. 8th). It is crucial to EASE into training, slowly building up, and maybe even starting with a couple rest days when arriving (Chapman et al., 2010). It will take about 5-7 days before the initial “shock” of being at altitude decreases. This exaggerates the importance of recovery, not only for when you are spending time at altitude but also when returning to sea level. Even elite runners have been known to take a full month to get back to their previous level of training at sea-level after altitude exposure (Greg McMillan, coach in Flagstaff). Once beginning high intensity training after several days of acclimatization, be careful to the recovery between intervals. It is recommended to use an exercise-to-rest ratio of 1:2 (2 min on and 4 min off) where at sea-level you can perform 1:1 (4 min on and 4 min off). Adjust the pace of threshold/temp work, as well as interval pace. It is important to slow down and take this seriously to allow time for the body to adapt (example in running, suggested to adjust 1 (or more) seconds per 400 m, 4-5 seconds per mile per 1000 ft above 3000 ft elevation). In addition, Hamlin et al. 2015 suggested that pacing should be adjusted from 800 m and higher, and that performance is 2-4% slower above 1000 m/3000 ft, and more than 4% slower above 2000 m/6000 ft.
Why? What causes our body to react differently at altitude?
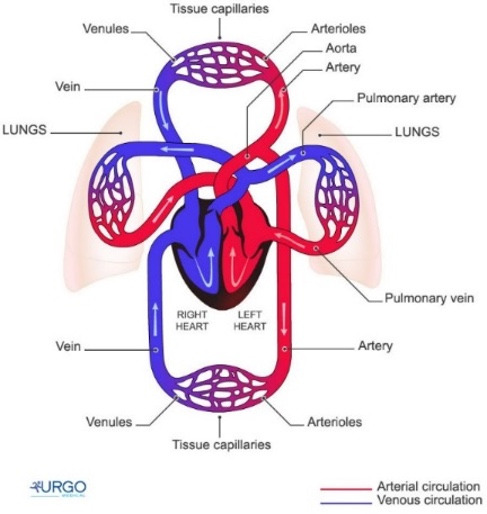
When traveling or climbing to higher elevation, there is progressively a different oxygen environment. The higher you go, the less oxygen is available (hypoxia) due to decreased air pressure in the atmosphere, therefore, there are less and less oxygen molecules present in the air for us to breathe to begin oxygen transport to our working tissues and our body can be greatly stressed. This reduction in oxygen delivery (oxygen transport from lungs all the way to the bloodstream) occurs resulting in insufficient oxygen availability at the tissue level where the body must respond to maintain a homeostatic balance (Lundby et al., 2009; Amann, 2011). One of the first processes that begins is in the kidneys, which communicate with the bone marrow to produce more red blood cells (and more hemoglobin, the oxygen carrying molecule in the blood) while also increasing the plasma volume to balance this process in the blood (Berglund, 1992).
What happens in the body at altitude?
In hypoxic conditions, there is a lower oxygen availability, and thus, a compensatory vasodilation (widening of vessels) induced by hypoxia. This vasodilation allows for a greater amount of blood flow to get more oxygen to the tissues. This is an autonomic response of the body, which involves interactions of metabolic and endothelial substances as well as mechanical factors which affect the vascular tone of the vessel, ultimately regulating blood flow to provide adequate oxygen delivery (Casey and Joyner, 2011).
Despite this happening, there are several physiological components which are greatly stressed by this hypoxic environment such as increased ventilation, increased cardiac output (product of heart rate and stroke volume, as the rate and strength of the heart), limited tissue oxygenation, shallow breathing which leads to respiratory alkalosis or a pH imbalance with the product being increased urination (contributing to dehydration), dehydration from dry and low level of humidity in environments, interrupted sleep in the first 3 weeks, etc. (Chapman et al., 2010, Sinex and Chapman, 2015). During maximal testing between 1,000 ft and 9,200 ft, researchers have demonstrated that VO2max decreased by a linear 1.9% for every 1,000 ft above 1,000 ft, as well as decreases in time to exhaustion by 4.4% for every 1,000 ft (Wehrlin and Hallén, 2006).
Exposure to altitude (both in severity and in increased dose/duration) results in tremendous effects at the cerebral level. The limited oxygen supply along with the brain’s limited ability to store glucose and other nutrients places stress on the regulation of cerebral blood flow (CBF). Acute exposure to hypoxia causes hyperventilation and therefore induced hypocapnia (low partial pressure of CO2), leading to vasoconstriction (narrowing of vessels) which affects the amount of vasodilation (widening of vessels) possible due to the low partial pressure of oxygen in the altitude environment (Ogoh et al., 2013). Regulation of CBF is crucial for maintaining oxygen delivery, as cerebral deoxygenation has been considered as an influential factor for decreasing exercise intensity or cessation of exercise (Smith and Billaut, 2010). Furthermore, low brain oxygenation due to insufficient blood flow and/or a lower oxygen concentration influences the delivery of oxygen to the mitochondria (powerhouse of cell, producing energy), which may induce a central fatigue (Kayser, 2003; Subudhi et al., 2007; Amann and Calbet, 2008). These factors together demonstrate the importance of adjusting pacing strategies to prevent overexertion and central limitations of performance.
With sufficient adaptation or acclimatization to altitude, there can be increased red blood cell mass and increased hemoglobin mass to bring more oxygen to the tissues. This leads to decreased sensation of effort, improved metabolic efficiency, and increased economy in movement (Saunders et al., 2004).
What can we do in order to prevent and adjust to these effects?
Prior to arriving at altitude, it is important to have a good period of training and feel strong regarding cardiovascular fitness. Performing regular sessions of high intensity training including intervals and hill training is advised.
Once in the environment, there are few dietary recommendations which can assist your body in this adjustment. Increase iron stores by eating iron-rich food sources (dark leafy greens such as spinach, beans and lentils, nuts, baked potatoes, etc) and increase carbohydrate intake above that of sea-level to adjust for increased energy requirements (Katayama et al., 2010). Pay special attention to your hydration status and drink more fluids, as there is greater fluid loss at altitude resulting from shallow breathing in addition to the dry environment. A crucial tip is to make sure to take extra rest, sleep well and take a daily nap (even if just 20-30 min). We need more sleep at altitude to make up for night sleeping interruptions which are present in the early stages of altitude exposure.
As far as training and exercise goes, SLOW DOWN and adjust your pacing strategies. This is especially important in the first 3-4 days upon arrival, maybe longer. It can be very helpful in this environment to use morning heart rate as a recovery monitoring tool (see Training Periodization : Monitoring Recovery posted on Nov. 8th). It is crucial to EASE into training, slowly building up, and maybe even starting with a couple rest days when arriving (Chapman et al., 2010). It will take about 5-7 days before the initial “shock” of being at altitude decreases. This exaggerates the importance of recovery, not only for when you are spending time at altitude but also when returning to sea level. Even elite runners have been known to take a full month to get back to their previous level of training at sea-level after altitude exposure (Greg McMillan, coach in Flagstaff). Once beginning high intensity training after several days of acclimatization, be careful to the recovery between intervals. It is recommended to use an exercise-to-rest ratio of 1:2 (2 min on and 4 min off) where at sea-level you can perform 1:1 (4 min on and 4 min off). Adjust the pace of threshold/temp work, as well as interval pace. It is important to slow down and take this seriously to allow time for the body to adapt (example in running, suggested to adjust 1 (or more) seconds per 400 m, 4-5 seconds per mile per 1000 ft above 3000 ft elevation). In addition, Hamlin et al. 2015 suggested that pacing should be adjusted from 800 m and higher, and that performance is 2-4% slower above 1000 m/3000 ft, and more than 4% slower above 2000 m/6000 ft.
How to approach a race at altitude? (based on Beidleman et al., 2017; Chawla and Saxena, 2014; Chapman et al., 2010)
- If short on time, the best may be to arrive right before the race. Arriving the “Day of” means to arrive the day of the race or within 24-48 hours before the race. This gives the body a limited chance to adapt and the effect/stress of altitude is often less. Plasma volume decreases 10-25% in the first arrival hours to altitude (Beidleman et al., 2017; Chawla and Saxena, 2014) and this can be a moment to capitalize before the body adjust for a homeostatic balance.
- Arriving 2-3 days before the race gets the “worst” part of the initial effect out of the way (however, this is tricky for adequate/essential recovery time). While 3-5 days before the race is recommended for a race around 1,640-6,560 feet.
- Traveling to altitude more than 7 days prior to the event is even better to get through the initial adjustment to living at altitude, while 1-2 weeks is recommended before a race between 6,560 – 9,840 feet.
- Ideal acclimatization to altitude is 21-28 days prior to the event to adjust and acclimate the body, especially in the blood, to being able to perform at altitude (≥ 3 weeks is recommended for races above 9,840 feet).
- Heat training at sea level can give great adaptations and a similar stimulus of adjusting plasma volume, though without the hypoxic effect of increasing red blood cell mass (White et al., 2014). This is a currently heavy researched area to better understand the possible crossover effects of heat and altitude training. In any case, it may be helpful in the adjustment to altitude to expose yourself to heat training in the period leading up to your travel.
Take home message = slow down and give yourself time for building up your training, eat well with more focus on iron, and pay attention to your hydration and sleep. Monitoring recovery helps understand when your body can handle more intensity and duration in training. Adjust your pace, especially in races that occur at altitude without sufficient time for acclimatization.
Stay tuned for Part 2 of this altitude series, which will focus on different altitude training methods.
References
Amann, M. (2011) Central and peripheral fatigue: interaction during cycling exercise in humans. Med Sci Sports Exerc 43(11), 2039-2045.
Amann, M., and Calbet, J.A. (2008). Convective oxygen transport and fatigue. J Appl Physiol (1985) 104(3), 861-870.
Bärtsch P., and Saltin B. (2008) General introduction to altitude adaptation and mountain sickness. Scand J Med Sci Sports 18 (Suppl 1): 1-10.
Beidleman, B. A., Fulco, C. S., Cadarette, B. S., Cymerman, A., Buller, M. J., Salgado, R. M., . . . Muza, S. R. (2017). Is normobaric hypoxia an effective treatment for sustaining previously acquired altitude acclimatization? Journal of Applied Physiology 123(5), 1214-1227.
Berglund, B. (1992) High-Altitude Training. Aspects of haematological adaptation. Sports Medicine 14, 289–303.
Chapman, R. F., Stickford, J. L., & Levine, B. D. (2010). Altitude training considerations for the winter sport athlete. Experimental Physiology 95(3), 411-421.
Casey, D.P., and Joyner, M.J. (2012) Compensatory vasodilatation during hypoxic exercise: mechanisms responsible for matching oxygen supply to demand. J Physiol 590(24), 6321-6326.
Chawla, S., and Saxena, S. (2014). Physiology of high-altitude acclimatization. Resonance 19(6), 538-548.
Hamlin, M.J., Hopkins, W.G., and Hollings, S.C. (2015) Effects of altitude on performance of elite track-and-field athletes. International Journal of Sports Physiology and Performance 10, 881-887.
Katayama, K., Goto, K., Ischida, K., and Ogita, F. (2010) Substrate utilization during exercise and recovery at moderate altitude. Metabolism Clinical and Experimental 59: 959-966.
Kayser, B. (2003) Exercise starts and ends in the brain. Eur J Appl Physiol 90(3-4), 411-419.
Lundby, C., Calbet, J.A., and Robach, P. (2009) The response of human skeletal muscle tissue to hypoxia. Cell Mol Life Sci 66(22), 3615-3623.
Ogoh, S., Sato, K., Nakahara, H., Okazaki, K., Subudhi, A.W., and Miyamoto, T. (2013) Effect of acute hypoxia on blood flow in vertebral and internal carotid arteries. Exp Physiol 98(3), 692-698.
Saunders, P.U., Telford, R.D., Pyne, D.B., Cunningham, R.B., Gore, C.J., Hahn, A.G., and Hawley, J.A. (2004) Improved running economy in elite runners after 20 days of simulated moderate-altitude exposure. J Appl Physiol 96: 931-937.
Sinex, J. A., and Chapman, R. F. (2015). Hypoxic training methods for improving endurance exercise performance. Journal of Sport and Health Science 4(4), 325-332.