
ANTERIOR KNEE PAIN (part two)
By Kurt Jepson,














Last month we discussed Infra Patellar Tendinosis, or “Jumper`s Knee”. This post will focus on another common origin of anterior knee pain, Patella Femoral Dysfunction (PFD).
Like “Jumper`s Knee”, PFD goes by many names such as; Patella Femoral Syndrome (PFS), Lateral Tracking Syndrome, Chondromalacia Patella and Patella Instability Syndrome. All denote biomechanical abnormality affecting proper kinematic function of the patella-femoral mechanism.
As discussed in part one, the Patella-Femoral Joint (PFJ) is designed to enhance the potential contractile abilities of the quadriceps muscle as it acts on the tibia via the moment arm involved. It is commonly agreed upon by most bio-mechanists that force production is enhanced approximately 30% via the PFJ. The PFJ also plays an important role in producing femoral rotation about a fixed tibia (during ground contact), as it translates lateral to medial across the condyles (bulbous ends) of the distal femur during knee flexion (Cleather D et al 2014). The knee is far from a simple “hinge” joint. Functional athletic movements about the knee require triplanar actions involving the patella, tibia and femur to maintain joint stability and convert muscle contraction into useful motion. Imagine trying to V1 up a steep hill without the ability to rotate your lower extremity relative to your pelvis, allowing for a powerful neutral platform proximally.
The compressive and shear loads encountered by the patella and femoral articular surfaces are extreme. Even small variances in mechanics over time can lead to “accumulation injury”.
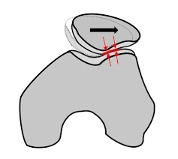
Most PFJ irritations arise from imbalances that lead to excessive lateral excursion of the patella as it translates along the femoral condyles during flexion/extension movements. This lack of ridge (patella) to groove (femur) congruency (centralization) causes focal loading, excessive compression and shearing of the articular cartilage surfaces.
Arthrokinematically, as the knee “bends” from an extended position, the patella translates medially and inferiorly (to the inside and down) from a relative supra-lateral (up and out) starting position. Different sections of the patellar surface bear load during this process. These sections are known as “articular facets”.
Flexed knee postures compress/load the central and medial zones and extended postures primarily load laterally. This will come into play when we discuss management strategies for PFJ symptoms.
Peripatellar tissue imbalances often result from lateral restrictions such as the IT Band and/or the lateral patella ligament complex (retinaculum). Correspondingly, medial “countering” tensioning may be compromised via an attenuated medial ligament complex (static) or quadriceps insufficiencies (dynamic). The fibers of the vastus medialis obliquus (VMO) are particularly vital to centralize PF position, as they insert at a near 60 degree angle on the patella. Any injury which inhibits the quadriceps (ie contusion) can lead to PFD over time.
There are many other contributing inputs to aberrant PFJ mechanics. Excessive transverse plane rotation of the tibia and femur due to foot pronation and gluteal weakness respectively, accentuate lateral patellar excursion and compression. This site has posted prior articles related to these topics and a review is suggested.
Lateral aspect of knee
Traumatic loads which displace the “kneecap” medially, or “sub lux” it, can acutely injury the articular cartilage of the femur and/or patella. Complete dislocations of the PFJ often require an ER visit, anesthetized reduction and prolonged immobilization. Resultant chondral injuries can require surgical intervention to debride loose fragments, stimulate healing and repair the medial stabilizing ligament complex. The incidence is approximately 6 per 100,000 episodes of injury in adults and 31 per 100,000 ages 10 to 19 (Stefancin J et al . Clin Ortho Relat Res . 2007).
More commonly, Patella-femoral symptoms result from overuse or training error (ie deep heavy squats, lunges plyo`s, bounding, etc). Non traumatic PFD symptoms typically include “snapping” or “grinding” (crepitus) when climbing stairs or arising from a chair. Stiffness when seated for long durations, for example car rides, is known as a “theatre sign”. A sense of quadriceps weakness and pain regionalized “behind” the kneecap is often described. Concurrent IT Band symptoms are common. Pain origins have been studied extensively and as referenced in part one of this series, are likely related to surrounding bursal and synovial tissues, as the cartilage surfaces themselves are aneural (Dye 1998). Unfortunately, articular cartilage is also avascular, making “healing” of friction induced lesions unlikely in adults.
Diagnosis of PFD involves acquiring a detailed history including current training load and any recent variations in terrain, shoe wear, gym work, or other potential inputs. Past trauma or operative history may be pertinent.
Physical exam involves provocative and alleviatory maneuvers as well as differential exclusion of other possible pain sources. Simple radiographs provide information regarding the presence of pre-mature arthritic change resultant of prior trauma. Positional asymmetries of the patella as it relates to the trochlear groove of the femur, and anatomic variants such as a shallow groove or non-prominent patellar ridge, calcified fragments, cysts, or spurs can all be ascertained via simple X-ray.
Below: “Sunrise view” of the PFJ with mild medial femoral condyle arthritis and a large projection “spur” off the lateral facet patella.
Palpation of the medial or lateral patellar borders to determine which is more tender, often correlates to load accumulation. Positional sensitivity during quadriceps contraction can also be confirmatory for either medial or lateral involvement. For example, if the medial aspect of the patella is most tender and is reactive to quadriceps loading while the knee is flexed past 60 degrees (ie lunges, full squats, quad extension machine), this is pathognomonic for medial PFJ compression syndrome. Conversely, if the lateral aspect is most tender and it hurts to do a loaded straight leg raise, or a standing lock out maneuver one may suspect lateral compression syndrome.
Recall that the retropatellar, (“behind”) surface of the patella bears compressive load central medially in flexed postures and laterally when extended. Any factors that alter normal tracking such as tight lateral structures “dragging” the kneecap to the outside (IT Band), poor hip strength, and/or a lack of offsetting medial dynamic inputs from the quadriceps VMO fibers can result in lateral excursion and frictional entrapment of surrounding soft tissue. This is a somewhat simplistic view, but demonstrates how vital soft tissue balance is to PFJ mechanics.
To manage PFD, the athlete must first negate any offending activities in the gym or while skiing (ie hill intervals).
Exercises must be selected that adequately stimulate the quadriceps in a neuromotor sense but do not add to pathomechanical stress. Overall PFJ compression peaks in flexed knee positions (+/- 90 degrees) during leg press and squat/lunge activities (”closed chain” exercise) and is conversely greater in full knee extension positions as the foot moves through space (“open chain” exercise). The median load intersection of these two forms of quad exercise occurs at 48 degrees per one study (Biomechanical considerations in patellofemoral joint rehabilitation. Steinkamp LA, Dillingham MF, et al. Amer J Sports Med, 21(3) 1993).
Quadriceps resistance should always be selected keeping the above premise in mind, as to not induce supraphysiologic forces during rehab. Heavy, deep squats or 20lb straight leg raises rarely go well for the patella!
Knee angles utilized for quadriceps work should be specific to the injured zone. Exercise positions selected should load the “pulley” mechanism away from the involved patellar facets.
If the athlete`s PFD is thought to be a medial/central compression issue, all squats, lunges, hill intervals, and full motion quad extension lifts need to be curtailed. This would be a good time to focus on DP, upper extremity strength, and non-weight bearing core exercise.
If symptom origin is believed to be laterally based, exercises where the knee is brought to, or held in full extension under load would be problematic. Examples include; single leg RDL`s, straight leg raises, terminal (30-0 degree) leg press work, step ups, side lunges or bounding to a fully extended end position, etc. These activities should all be avoided in the initial phase of rehab if dealing with a lateral compression problem as they potentially load the lateral facet or entrap surrounding soft tissue.
Global quadriceps weakness and atrophy, inevitability present, must be addressed to allow for balanced function of the PFJ (Giles LS et al. Atrophy of the Quadriceps Is Not Isolated to the Vastus Medialis Oblique in Individuals with Patellofemoral pain. JOSPT. 2015). A detailed retrospective look at 15 studies focusing on treatment approaches for PFD published in the Dec 2014 issue of Physical Therapy, definitively identified pathology specific hip and knee exercise as the most efficacious intervention for an individual with PFD. Clinical interventions in the absence of exercise had poor outcomes. The athlete must regain full quad function to resolve PFD symptoms. The trick is selecting non provocative modes of exercise.
As PFD involves “shearing” load intolerance as the patella glides over the femoral condyles, early quad exercise is best done isometrically and in a joint position not associated with irritation. This might include “light” (25-50% effort) 60-30 degree isometrics while seated against a resistive band, or on a quad extension machine for lateral compression issues.
For medial compression symptoms, supine straight leg raises with a 1-5lb ankle weight held 10-20 seconds should be initiated. Terminal extension (0-30 degrees) lateral step ups, perhaps holding a dumbbell, will likely be tolerated. Cycling and pool activities can help maintain general fitness.
Below: quad iso`s in relative flexion, painless 10-30 sec efforts, 6-10 reps (for lateral patellar symptoms)
Classic SLR exercise, 1-5lb ankle wt. ,10-30 sec efforts, 10-20 reps (for medial patellar symptoms)
Hip abductor and rotator work, are essential to a favorable outcome.
As the PFJ gains tolerance for graded exercise, the athlete can shift from range specific open kinetic chain (OKC) exercise to more functional closed kinetic chain (CKC) postures for isometric quad loading. The same focus on painless, non-provocative knee angles for loading should continue in this phase.
Below: CKC iso loading, 30+ sec duration, 6-10 reps
The final stages of rehab include the logical addition of traditional lower extremity exercise involving balance, functional movements, multiple reps and sets, plyo`s, and finally a return to running and skiing. The process can take weeks, particularly if the issue is chronic. Be patient. This is not an injury one can successfully “train through”.
Thermal and electrical pain modalities, as well as OTC medicines, if appropriate, may provide symptom relief during rehab. Wraps, patellar supports and taping all seem to have anecdotal benefit but do not influence patellar tracking as often claimed (Callaghan M et al, JOSPT 2016, Logan C et al Sports Health 2017, Ho Kai-Yu et al JOSPT 2017). The forces involved are simply too great to affect with an external device or tape. There is some evidence they alter quadriceps firing patterns and there is no down side to their use in combination with exercise (Callaghan MJ, et al. JOSPT 2016).
Formal Physical Therapy may be necessary to manually “mobilize” tight patellar tissue or employ biofeedback techniques for proper sequential quadriceps activation. Lateral patellar “tilt” and deviation has been shown to be a major predictor for PFD by numerous investigators and should be addressed via PT if pronounced (Boden B, et al. J Am Acad Ortho Surg 1997 and Nunes G et al. Phys Ther in Sport 2013).
IT Band stretching and foam rolling are easily completed independently when indicated. Shoe design and orthotic use should be discussed. Very few non traumatic PFD situations result in surgical intervention.
Patella-femoral Dysfunction is extremely prevalent in the athletic population. It need not become an extended detriment to one`s training plans, provided it is identified early.
As you begin a new training cycle this spring and re-introduce modes of exercise you haven`t visited in a while, monitor any onset of anterior knee pain. Classify symptoms as “Jumper`s Knee” or PFD and take the appropriate steps to arrest it early, correct any contributing factors and pursue your training uninterrupted.