
LateRal Knee Pain (ITBS) - Why We Get It
By Kurt Jepson
In the sagittal plane the distal ITB moves from a relative anterior position when the knee is extended, to a posterior position as we flex the knee. Research indicates the maximal angle of compression against the prominent tibial plateau and lateral femoral condyle is approximately 30 deg of knee flexion. As the band migrates front to rear it experiences maximal friction in this 30 degree position (think wiper moving over a prominence on your windshield). Unfortunately, in sport, we pass through 30 degrees of knee flexion under load frequently. Running or skiing hills, stairs, lunges, plyo`s, etc. all have the potential to cause or elevate symptoms.


LATERAL KNEE PAIN- ILLIOTIBIAL BAND SYNDROME (ITBS), WHY WE GET IT.
It is very likely, as an endurance athlete, you have, or may experience pain with on the outside (lateral aspect) of your knee during, or subsequent to training.
There are of various potential reasons for lateral knee symptoms including but not limited to:
Early degenerative changes within the knee, lateral meniscal pathology, lateral patellar compression syndrome, or simple sprains, strains and contusions. However, in the absence of a traumatic input, swelling of the knee proper, or chronologic age where arthritic changes are a reasonable assumption, ITBS may be the cause of your pain.
ITBS can have a proximal hip component as well. This article will focus on the distal issue at the knee.
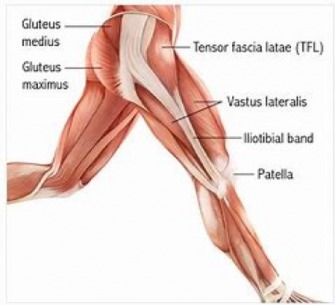
Anatomy:
The Iliotibial Band (ITB) complex consists of the Tensor Fasciae Latae (TFL) muscle which arises off the outer crest of our pelvis and courses down the lateral thigh. It transitions to more tendinous characteristics ( the “IT Band” ) prior to its insertion on the anterolateral tibia ( Gerdy`s Tubercle) just below the joint line.
Kinematics:
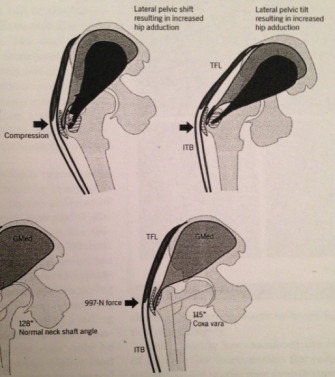
The ITB enhances lateral knee stability via passive and active inputs. It assists with hip and knee flexion based on the position of the hip and contributes to triplanar stability of the entire lower extremity during single leg stance activities. It is one of the “prime movers” of the limb laterally during hip abduction. The TFL comprises 10-15% of the total cross sectional area of the abductor muscles (Clark JM, et al J Bone Joint Surg Am., 1987). Its contribution to active hip abduction force is a combination of its contractile abilities and a passive fascial component. The TIB Tensioning Mechanism is thought to produce as much as 30% of the total force required to stabilized the pelvis when standing on one leg (Kummer B , Ann Anat 1993). The resultant compression and tensile loads are substantial.
(Grimaldi and Fearon, JOSPT, now 2015
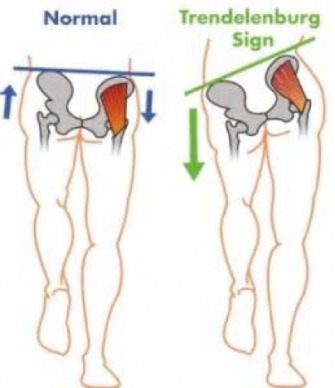
During the gait cycle and any single leg stance position such as gliding, the hip abductors must vigorously contract to keep the pelvis level and control rotation. Joint loads at the hip can be extremely high. Work by Stansfield BW, et al via indwelling strain gauges, demonstrated induced loads at the hip to be 3 times body weight while walking and 5-6 times body weight while running or using stairs (Clin Biomech.2002). Other investigators have published similar data. Failure to “dampen” these forces results in destabilization of the pelvis and core. All three planes of movement are affected.
In the sagittal plane the distal ITB moves from a relative anterior position when the knee is extended, to a posterior position as we flex the knee. Research indicates the maximal angle of compression against the prominent tibial plateau and lateral femoral condyle is approximately 30 deg of knee flexion. As the band migrates front to rear it experiences maximal friction in this 30 degree position (think wiper moving over a prominence on your windshield). Unfortunately, in sport, we pass through 30 degrees of knee flexion under load frequently. Running or skiing hills, stairs, lunges, plyo`s, etc. all have the potential to cause or elevate symptoms.
Pathomechanics:
As with most tendinous structures, the ITB complex is irritated by a combination of excessive tensile and compressive loading, typically at its origin or insertion. Given the information above it is easy to see that if the gluteal and rotator groups about the hip are unable (“weak”) or unwilling (“deactivated”) to deal with the forces generated via function, the TFL and ITB will come under load from the limb adducting and internally rotating. The (TFL) will vigorously attempt to generate compensatory abduction force and at the same time the ITB be overloaded from inward “collapse”.
Other predisposing architectural factors can contribute to pathomechanical inputs such as tibial varum (“bow legs”) which pre loads the ITB at Gerdy`s tubercle. On the other end of the spectrum, an excessive Q angle at the knee (“ knock knees”) and an overpronating foot contribute to dynamic internal and adduction moments of the entire limb at stance. The end result at the ski snow interface is poor glide and compromised propulsion.
Tibial Verum
High Q angle/Valgum
Management:
Iliotibial Band Syndrome treatment should address the specific components and predisposing factors of each athlete. Utilization of a “cookie cutter” approach will seldom produce favorable long term outcomes. For instance, an athlete with inward collapse of the limb during stance/gliding, a large Q angle and “flat feet” will not benefit from stretching, foam rolling and icing. They require core, gluteal and rotator strengthening and would likely respond well to an orthotic.
Conversely an athlete with “ high arches” while standing, varus legs and restricted hip motion may respond to stretching and mobility exercises. These athletes may benefit from foam rolling but this should only be incorporated into the sub-acute phase, as compression and tensile loading via rolling may actually delay resolution. Massage, ice, and anti-inflammatory medicines can be useful adjuncts. Always check with your health care provider before using pharmaceuticals. Knee wraps and sleeves are not recommended as they may actually increase compression inputs laterally.
Training mode, volume, intensity and terrain may require adaptation to allow the injured region time to negate inflammation, remodel, and build durability. You will need to make time to activate deficient proximal core and hip muscle groups. High cadence cycling with mild to moderate load is usually tolerated and will help preserve L1 fitness.
Lastly get qualified advice from your Sports PT, L-AT (athletic trainer) or sports fellowed Physician regarding running shoe selection. In my experience, “minimalist” training shoes have no place in the management of ITB Syndrome.
I my next article, I`ll go over specific rehabilitation exercises to address restrictions, weakness and movement pattern flaws. Check back!