
ILLIOTIBIAL BAND SYNDROME - PART 3
Lateral Knee pain / Illiotibial Band Syndrome, the “Hypomobile” athlete


Above is video of Ingvild Flugstad Oestberg of Norway, another very talented athlete. She represents the “hypomobile” variation for discussion purposes. I encourage you to review Stadlober`s concurrently with Oestberg`s.




By Kurt Jepson
This is the third in a series of articles focusing on the pathogenesis and management of a common cause of lateral knee pain in endurance athletes.
Illiotibial Band Syndrome (ITBS) may result from direct trauma to the lateral knee (contusion) but more commonly is the result of kinematic and/or training inputs. In part 2 we examined pathomechanical inputs to the Tensor Fascia Latae proximally and the ITB at it`s insertion distally. We focused on isolated weakness and resultant “undampened” loads in the “hypermobile” skier as contributing inputs.
Let`s look at the other end of the spectrum, the “hypomobile” athlete.
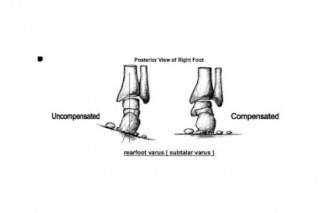
These individuals often present posturally with limited lumbar lordosis, neutral femoral orientation or slight retroversion (external rotation), genu varum (bow legs) of the knees, external tibial torsion and more restricted high arched feet often with accompanying tight calves. In pronounced variations, there is resultant “under pronation” in these individuals during the gait cycle. As a very small portion of the population actively “supinates” as a compensatory motion for mid foot alignment therefore, “under pronation”, is a more representative term for people in this category.
(Varus limb)
These combined characteristics result in a relative varus hind foot (calcaneal) position through much of the gait cycle. Lever systems are quite rigid and responsive (think sprinters feet) but at the cost of vertical load dispersion and the loss of a subtle adapter to adjust to terrain enhancing balance.
(Hindfoot Varus)
In skiing, less inward collapse (valgus) and greater ability to maintain the limb perpendicular to the ground (relative varus) equate to less inside edge loading during the early and mid -glide phase. This is obviously advantageous. However, if varus components are extreme, undesirable outside edge loading can occur. Very few people are “neutral” and it becomes a matter of degree one way or the other. Everyone seeks to ride that elusive “flat ski” and your ability to do so is in part postural driven.
(Valgus collapse)
The ability to recognize and adapt to these architectural characteristics via technique, exercise, and equipment variations (ie orthotics ) is what sets fast skiers apart from the rest of the pack.
In the previous segment we included video of Teresa Stadlober of Austria. It goes without saying she is a very talented athlete. Kinematically however she does demonstrate how relative valgus, weakness and hypermobility can influence technique and metabolic cost to maintain speed.
Above is video of Ingvild Flugstad Oestberg of Norway, another very talented athlete. She represents the “hypomobile” variation for discussion purposes. I encourage you to review Stadlober`s concurrently with Oestberg`s.
VIDEO LINK : (video also posted at the top of article)
Comparatively note Oestberg`s upright head and torso indicating a more neutral core. This allows for better hand positioning prior to her poling impulse, set her scapular musculature, enhance diaphragmatic function and assist with balance as she maneuvers her hips forward. From this upright position her hips have less distance to travel to get forward. They are readily accessible from this starting point thereby lowering her cost of movement.
Also, note Oestberg`s pelvis. It rotates very little front to back in the transverse plane nor does tip laterally in the frontal plane. This firm foundation allows the lower extremity musculature to generate significant extension and abduction forces to the snow, while dampening rotational motion.
Observe her patella just prior to placing the new glide ski on the ground. It is seeking a lateral position (varus), the result of an externally rotated femur as she prepares for the new stance leg. She is able to stand comfortably and balanced on her new glide ski assisted by a strong posterolateral column. Her knee stays in neutral (relative varus) through early and mid glide and only does it subtly “flick” into valgus prior to edge set.
With all of the positives listed above, how can there be any downside to having a “hypomobile” stature as a skier? The short answer is yes.
In terms of the ITB complex, a varus posture of the knee does expose it to frictional input as the prominent lateral tibial and femoral contours come in contact. In the first segment of this series we mentioned the 30 degree knee angle, as a point of maximum compression between the ITB and the lateral osseus components of the knee (Fairclough J, et al, J Anat 2006). Functionally we pass through this angle constantly as we ski. Varus knees (Genu Varum), a tight ITB/TFL complex, and repetitive flexion and extension, particularly under load, can result in lateral irritation. Lengthening of the ITB complex can lessen compressive loads.
An externally rotated extremity can also lead to functional shortening of the ITB complex further exacerbating compressive load proximally and/or distally. Tight external rotators of the hip and a dominant lateral hamstring (biceps femorus) can contribute to any structural tendencies.
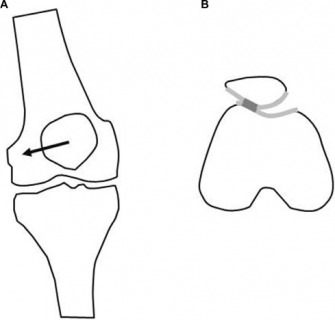
Lateral patellar compression syndrome via a mal-tracking kneecap often accompanies ITB tightness as it`s insertional fibers blend with the lateral patellar retinaculum fibers. Restrictions induce lateral tilt and shift of the patella. The kneecap serves as a pulley mechanism for knee extension increasing efficiency by 30%. Retropatellar compressive forces are significant and if lateral translation occurs during it`s function, symptoms of pain and “cracking” (crepitus) develop.
(Lateral patellar tracking)
Hindfoot varus, subsequent to tibial varum, contributes to Achilles restrictions. An article posted in November discussed the repercussions of a skier having calf tightness. Functionally we compensate for calf/Achilles tightness via pronation (refer to part 2 to review ITB consequences).
Anatomic or functional leg length discrepancies (due to lumbosacral dysfunctions), can also have adverse inputs to the ITB. “Long” limbs “shorten” via pronation. Conversely “short” limbs maintain supination/ varus posture of the heels and knees throughout the gait cycle limiting medial edge set (SK) and great toe loading (CL) .
Lastly, those athletes whose genetic morphology lends to more rigid structure typically have less flexibility than those that are highly mobile. Muscle restrictions may increase the metabolic cost of movement as “prime movers” (agonists) work against external loads, as well as opposing muscle (antagonistic) restrictions.
MANAGEMENT:
In part 2 we focused on activation and strengthening exercises for the “hypermobile” athlete. We certainly want to include these same activities with the “hypomobile” athlete discussed here but will also add flexibility and tissue interface mobility to the plan (assuming no lumbar disc or structural knee issues).
Posterolateral stretching;
ITB TFL Stretching;
Foam Rolling (avoid excessive bony compression);
Further treatment of acute or chronic ITB Syndrome may include; anti inflammatory medicines as approved by your physician, PT modalities, manual tissue work, cryotherapy, taping procedures, foot orthotics and of course activity modification. Unfortunately, the literature is somewhat unsupportive of these interventions (other than therapeutic exercise) in terms of efficacy (Cochrane Reviews, nov 2014). Anecdotally patients report good tolerance and benefit particularly when used in conjunction with corrective exercise.
In conclusion, Illiotibial Band Syndrome is a common malady of the endurance athlete. Understanding the individual`s contributing factors of lateral knee pain is paramount. Addressing structural, kinematic, and training flaws as opposed to just treating symptoms will help negate the inflammatory process, provide prophylacsis and enhance performance.