
ROLLER SKI INDUCED ELBOW PAIN
By Kurt Jepson





Shoulder and core exercise may continue as long as the athlete does not grasp the apparatus during the resistive movement and rather uses their fore or upper arm as the main contact point. Pulley work may continue if the point of resistance is proximal to the wrist so the flexors and extensors are by- passed. Some examples are shown below.








During late summer and autumn, it`s likely many skier`s training plans include a transition to more intensity and pace work while utilizing roller skis. As a result, the load placed on forearm musculature and associated skeletal structures may exceed their tolerances via cyclic or singular force inputs. Medial (inner/ulnar) or lateral (outer/radial) elbow pain can develop gradually or acutely. Barring traumatic input such as a fall or direct blow, Medial Epicondylitis/ “Golfer`s Elbow” or Lateral Epicondylitis/ “Tennis Elbow” is often the diagnosis. Quickly assessing the problem and more importantly avoiding it, can prevent weeks or months of aggravation and adapted training.
“Epicondylitis” describes an inflammatory process occurring at the tendon/ bone origin of the wrist/finger flexors/pronator groups (medial) or wrist/finger extensors/supinator groups (lateral). It is more accurately described as a “tendinosis” or “tendinopathy” as histologically the structure undergoes a process of repetitive micro tearing and an incomplete reparative response (Ciccotti et al 2004). As such it becomes a structural problem. It was first described in 1882 by Morris as “lawn tennis elbow”. Lateral epicondylitis has garnered the majority of research since first described, and occurs 7-10 times more frequently. The pathophysiology and management strategies for both maladies are generally agreed upon to be similar in nature.
ETIOLOGY
Epicondylitis is typically the result of forceful cyclic loading via repetitive impact, grasping or lifting. The load associated with using a” jack hammer” is often used as an example of pathomechanical input to the epicondylar regions. Forces involved with roller skiing would seem to follow suit. Glazebrook et al measured the EMG activity of the forearm flexor pronator group during a golf swing and noted a mean 90.8% of max volitional contraction (MVC) force just prior to, and at ball contact (Medial Epicondylitis, An Electromyographic Analysis and an Investigation of Intervention Strategies, Amer J Sports Med , 22(5), 1994). They coined the phrase “flexor burst” to reinforce how violent the extrinsic load, and subsequent muscle contraction can be especially when delivered cyclically.
That`s a golf club hitting a ball, imagine the force when pole tips hit the ground during ski intervals!
Despite the associated nicknames, Epicondylitis is far more prevalent in the industrial work setting than athletics. One study reported it comprised up to 64% of all industrial workplace maladies (Dimberg L, Ergonomics 30: 1987). Most cases (83-90% per Smidt et al, J Rheumatol 2006)) resolve within a year by avoiding the offending activity and only 5% go to surgery (Karhanis et al, Br Med Bull 2008). The sticking point with athletes is of course, interrupting normal training for a year.
ANATOMY
The anatomy of the two regions is presented below;
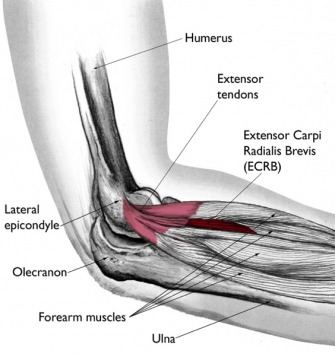
LATERAL EPICONDYLAR / COMMON EXTENSOR REGION
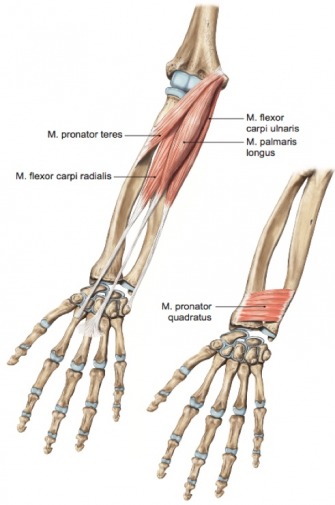
MEDIAL EPICONDYLAR/COMMON FLEXOR REGION
Of note in both regions is the relatively short, shared and nondescript tendon structure which does not allow for force dispersion generated by associated muscle groups. This concentration of load, along with tendons being relatively avascular in nature, predispose the” Common Flexor” and “Common Extensor” tendon bone interface to mechanical failure, ineffective healing and re-injury.
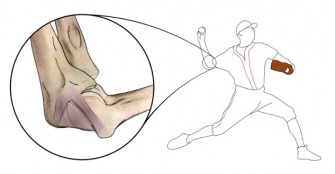
Not depicted above is the extensive ligamentous and neuro vascular anatomy which can cloud the diagnostic picture and complicate some injuries. The medial side in particular is prone to ligamentous injury and ulnar nerve irritation via repetitive valgus and extension motions such as those encountered in throwing and racket strokes. Medially the tendinous fibers blend with the ligamentous complex and stress on one translates to the other. “Little Leaguers Elbow” is a common problem in young throwing athlete`s resultant of medial elbow angular induced stress.
The stress to the medial elbow during pole strike in quite similar kinematically, specifically an abrupt valgus/ “opening” load placed on the stabilizing soft tissue. Poling also involves vigorous grasping and pronation (pole release) at the termination of the movement, much like ball release.
MUSCLE ACTION
As the names imply, the Common Extensors straighten or extend the digits, the wrist and a related muscle supinates (palms up) the wrist/hand complex. Conversely the Common Flexors Pronators bend the digits, flex the wrist and pronate (palms down) the wrist/hand complex. Both groups contract vigorously during grasping. Tension transmitted to their respective tendinous attachment is relative to the contractile force generated.
DIFFERENTIAL DIAGNOSIS
As with any musculoskeletal issue which is resultant of trauma and/or persists for many days without signs of improvement, medical assessment is appropriate. Elbow pain can be driven by fracture, post traumatic arthritis, nerve entrapment centrally or peripherally, neoplasm, ligamentous instability, or growth plate pathology in a skeletally immature athlete.
PREVENTION AND MANAGEMENT
In the symptomatic athlete the interventions should match the phase of the tendinosis. There are 4 basic phases of involvement as described by Noteboom et al ( Tennis Elbow a Review, JOSPT vol 19, 6, 1994) which drive focused treatment.
1. Inflammation (~0-10 days). Implementation of anti-inflammatory modalities is useful to assist with pain and dampen the bodies excessive “healing response”. Ice cup massage, electrical stimulation, iontophoresis (topical delivery of steroid), oral non-steroidal medicine and provocative activity avoidance are recommended. Studies by Kivi, Halle and others have shown no long term benefit to steroid injection. Low load, high rep exercise of the “uninvolved” region of the elbow can begin ( ie wrist curls if one has Lateral Epicondylar symptoms) provided it does not include vigorous grasping. Remember, tendinopathies are resultant of compression and/or tensile load intolerance and compromised cellular health. Stretching that structure prior to maturation is contraindicated and will only delay resolution.
2. Tissue Healing and early Organization (~1-3 weeks). The goal in this phase is to provide a conducive environment for cell growth and maturation. Circulatory enhancement to a relatively non vascular region is key. Electrical modalities, self or professional massage and contrast thermal packs all enhance circulation and should be used multiple times daily. Focused Transverse Friction Massage, tool based soft tissue release work, taping procedures, and dry needling have mixed efficacy per Cochrane Review (Issue 1 2006) but anacdotally have been used for years with success and do no harm. Brattberg et al (1983) found acupuncture useful in symptom improvement in 60%+ of patients who failed cortisone injection. A likely mechanism for this success was the circulatory response to “peppering” the region with micro trauma via needle sticks.
I find friction massage is very useful and easily performed independently with a thumb. It should be utilized daily for 7-10 days once the area is “sub-acute”. A duration of 5 minutes is typical. The elevation in discomfort should follow the same guidelines as those listed for early exercise below.
Exercise in phase 2. should revolve around daily sub maximal isometrics (10-50% perceived effort) which are sustained in duration (60-90 seconds) and low in repetition (2-4). They should elicit no more than an analog pain scale (0-10) increase of 2 additional levels above ones resting pain. For example, if you are a 2/10 at rest regarding your discomfort, treatment should elicit no greater than a 4/10. Any residual elevation of symptoms should resolve within 12 hours. If it lingers, intensity and frequency should be adjusted accordingly. Exercise bands or small weights can be utilized.
Wrist flexor sub max isometric holds for Medial Epicondylar involvement. 60-90 sec x 4 reps, 1-5 lbs or light exercise band suggested.
Above; Digit extension isometric`s for Lateral “Tennis Elbow” symptoms. Hold time 60-90 sec x 4 reps daily. Ball squeezing using the same format would be an option for Medial “Golfer`s Elbow” symptoms.
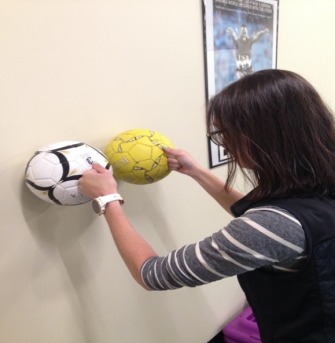
Shoulder and core exercise may continue as long as the athlete does not grasp the apparatus during the resistive movement and rather uses their fore or upper arm as the main contact point. Pulley work may continue if the point of resistance is proximal to the wrist so the flexors and extensors are by- passed. Some examples are shown below.
The provocative activity (ie poling) must continue to be absent from training. It`s a good time to no pole ski and work on your core.
3. Muscle Conditioning (~3-6 weeks). In this phase the focus is on normalization of functional strength. If there is motion loss about the wrist stretching exercise can now occur. Isometrics (50-100% effort) can be reduced to 2-3x weekly to ensure the tendon complex has sufficient stimulus to increase tensile competence. Traditional wrist curls, cock ups, radial deviation (thumbs up curls), etc. should focus on ECCENTRIC work. Eccentrics are characterized as a controlled lengthening on the muscle fibers as they resist the applied load (controlled lowering of the weight). Up with help, down slow, are cues to the movement.
The literature is overwhelmingly clear on the value of eccentric vs. concentric exercise for mid and end stage management of tendonitis anywhere in the body, and specifically Epicondylitis (Tyler et al, Inter J Sports Phys Ther 2012, Foidart-Dessalle et al, J Sports Med 2007, Stassinopoulos et al Hand Ther 2017 ,etc). Eccentrics stimulate the fiber matrix within the tissue to withstand tensile load, increase the collagen building “ground substance” and improve vascularity. Four Sets of 8-15 reps are typical with a load that again honors the “no more than 2 levels of pain” jump from the resting state on a 10 point analog scale. Exercise tubing is very useful for this mode of exercise. Use the opposing hand to assist the involved side into the “up position” and then remove the help and slowly lower against the force (3-6 sec per effort).
Assessing grip strength and comfort is a simple way to judge progression. The finger flexors generate the majority of force during grasping but the extensor group must co-contract with equal vigor to maintain a neutral posture of the wrist during the task. Pain will result from a muscle tendon unit unable to tolerate tensile loads and grip will lessen reflexively via neuromuscular inhibition.
A goal of the dominant hand being 5% stronger than the non-dominant is reasonable.
Easy DP work can resume within the later part of this phase based on symptoms, acceptable grip strength. The athlete should follow a logical progression of exposure to duration and intensity.
4. Controlling/Dampening Force Loads (~6 wks- 6 mos). Extended durability and prevention are the focus of this phase. Epicondylitis has a fairly high recurrence rate due to incomplete or rushed rehabilitation. Wrist and forearm exercise should become a bi-weekly part of one`s training program. Traditional reps and sets can be reinstated, but a least 2 sessions per month should work on maximal load (ie 4 sets of 4 reps “heavy”) to ensure tissue stimulus for tensile durability is ongoing. Your high rep endurance training needs will be met when you go skiing.
Equipment should be inspected and adapted as necessary. Composite poles may dampen more load at tip strike than 100% carbon shafts. Tips should be sharp as “slipping” under load adds to reactive contractile forces. Straps should be sized accurately to allow smooth release and recovery. This improves blood flow at the epicondyles during the relaxation phase of pole swing.
Elbow sleeves in cool weather may help. Counterforce armbands and taping have mixed support in the recent literature but older studies did find that pain, extensor strength and grip all were enhanced via the use of “Tennis Elbow” straps on a symptomatic limb (Wadsworth et al 1989, Vicenzino et al 2003, Groppel et al 1986 , Synder-Mackler et al 1989). They will do no harm if used properly.
End stage exercise focusing on “stacked” neutral control of the wrist requiring forearm co-contraction.
Counterforce armband Size your wrist straps appropriately.
Elbow tendonitis would seem a relative “non-player” in terms of lost training time but anyone who has battled it can tell you it is quite debilitating. Epicondylitis is best addressed via prophylactic training (just combine step 3. and 4. components into your weekly dry land sessions), early recognition, and proper management if afflicted.
Enjoy the change of seasons!