
ANTERIOR KNEE PAIN (part one)
By Kurt Jepson




There is likely no more frequently encountered lower extremity malady in sports medicine practice than “anterior” (frontal) knee pain. It spans all age groups, athletic categories and gender. Etiology ranges from traumatically induced injury, training error, inadequate fitness levels and infrequently, disease processes. Most cases are benign and resolve favorably with conservative management if properly diagnosed and classified. That said, anterior knee pain (AKP) can interrupt an athlete`s training or competitive seasons.
Diagnoses of AKP include a hodge-podge of nonspecific descriptives, but few of these speak to anatomic structure or pathogenesis. Examples include; Patella Femoral Dysfunction, Lateral Tracking Syndrome, Runner`s Knee, Jumper`s Knee, Nurse Maid`s Knee, and Lateral Compression Syndrome. Some diagnoses such as “Chondromalacia” are provided prematurely and without specific data, such as imaging or arthroscopy.
Because of the expansive volume of information associated anterior knee pain, this article will be broken into two parts. In part one, we`ll look at the functional anatomy and discuss Patellar Tendinitis (Jumper`s Knee). In a subsequent posting Patellar Pain Syndromes and Patellar Instabilities will be addressed.
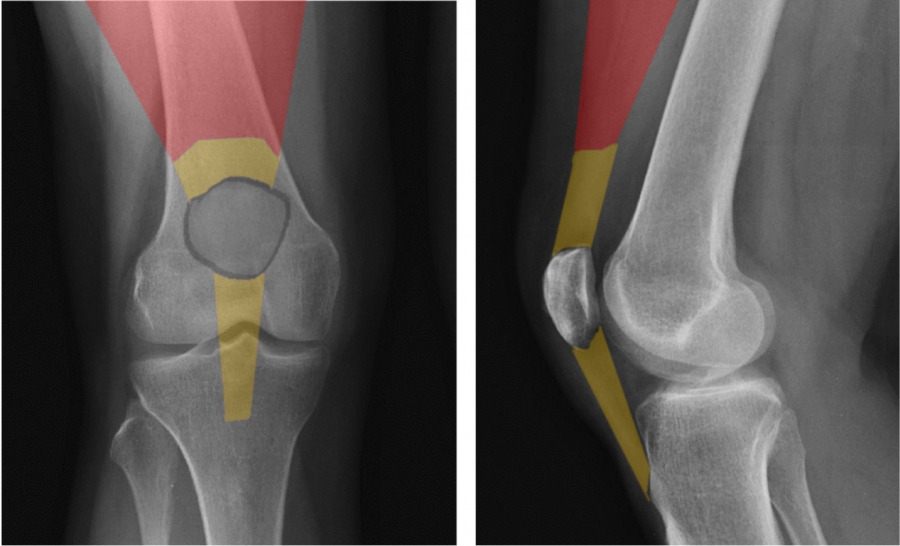
The Quadriceps mechanism includes a complex arrangement of muscular, tendonous, bony, synovial (membranous) and bursal tissue. The quadricep`s muscle comprises the majority of surface area of the frontal thigh and distal anatomy includes the patella and associated ligaments and tendons. Synovial and bursal tissue surround all structures to provide “frictional protection” for adjacent tissue layers and/or nutrient supply for hypovascularized regions.
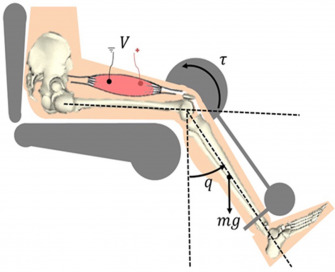
The patella is classified as a Sesamoid bone, meaning it is encased within a tendon. It`s purpose is to serve as a mechanical “pulley” for the quadriceps during it`s action of knee extension. It improves net force production by approximately 30%.
The patella is apically shaped and it`s undersurface, or articular surface, is coated with thick hyaline cartilage to reduce friction as it glides over the distal femoral condyles, also coated with cartilage. When you disarticulate a chicken leg, the white “shiny” surfaces of that joint complex is articular cartilage.
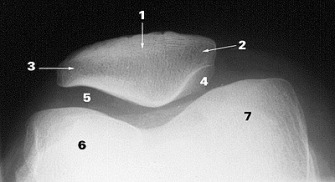
The “retro patellar” (under) surface has a central prominence or ridge, designed to “track” within the central groove created by the two femoral condyles (6 and 7). The patellar under surface is also divided into 4 articular “facets” (medial 4, lateral 3, central, odd 2). Each facet has a range of motion dictated role in absorbing compressive loads as it operates as a pulley. The lateral facet absorbs load in extension of the knee, and correspondingly the medial and odd facets during flexion. Compressive loads between the femur and patella can be enormous, often hundreds of pounds (Cohen et al, Amer J Sports Med, 29 (4), 2001 and Powers et al, J Ortho Sports Phys Ther, 44, 2014). To accommodate these loads, the “retro-patellar” articular cartilage is the thickest in the body, approaching 7mm along the central ridge (Ahmed et al, J Orthop Res, 1987). Despite the durability of the patella, surface lesions do occur and unfortunately the hypo- vascular nature of articular cartilage restricts healing once damaged. Surrounding patellar ligament complexes including the Medial Patella Femoral Ligament (MPFL) medially and the Lateral Patellar Retinaculum help guide centralized patellar movement. They also provide stability against “dislocating” forces.
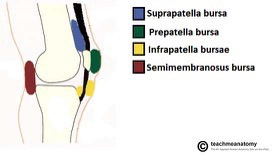
Bursal sacks form interfaces between adjacent tissues that may “rub” on each other during movement, thus creating a buffer to frictional inputs. Internally, synovial membrane secretions help nourish the micro vascular environment. Unlike the cartilage components, these membranes are highly innervated and thought by many to be the source of most AKP (Dye SF, Vaupel GL, Dye CC. Conscious neurosensory mapping of the internal structures of the human knee without intraarticular anesthesia. Am J Sports Med. 1998; 26:773–777).
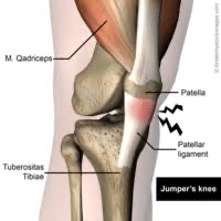
Infrapatellar Tendinitis or “Jumpers Knee” is a common form of AKP. The Infrapatellar Tendon (below the patella) is considered “ligamentous” by some, as it connects bone to bone (patella to tibia).
As with most tendonous injuries, the cumulative affects of excessive tensile and compressive loads can lead to structural compromise and anomaly. Exercise movements, loads and repetitions that the athlete is unaccustomed to, can reduce tendon stiffness and cause microcirculatory compromise (ischemia) within the tendon matrix (Lian OB, et al. Prevalence of Jumper`s Knee.
Among Elite Athletes from Different Sports: A Cross Sectional Study. (33) Am J Sports Med 2005). Even small partial failures of tendon tissue in animal models triggered histologic abnormalities and functional compromise which persisted for 12 months in a study by Scott A et al, J Ortho Res ,2011.
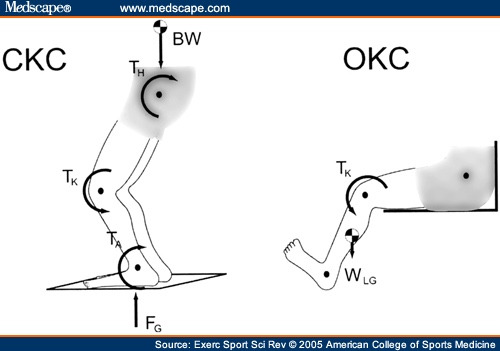
Infrapatellar injuries can be chronic and very frustrating. As the radiographic diagram above indicates, the infrapatellar tendon comes under “stretch” load as the knee flexes. When a vigorous quadriceps contraction occurs, stretch load is greatly accentuated by muscle induced tension as the quad acts on the tibia. Forces are particularly high in the tendon during “rapid load storing and release” activities (i.e. plyometrics). Eccentric activities can have either an injurious or reparative affect based on dosage. A review of a previous Nordic Solutions post entitled, “The Role of Eccentric Exercise in Early Season Training” is recommended.
Histologically, an injured infrapatellar tendon is comprised of thinner collagen fibers which are less directionally organized. Proteoglycan concentration is higher, as is water content within the tissue matrix. Blood vessels and sensory nerves are more concentrated, lending to a pain response. There are areas of cell death and fibrosis indicating ongoing healing attempts (Brukner P , Khan K, Clinical Sports Medicine, 2006). Calcifications may be present in chronic cases. Overall, the tendon is thicker in diameter but less able to tolerate tensile loading due to the structural changes noted above.
An athlete with “Jumper`s Knee” will typically limp during running, or bounding activities. When skiing, the athlete will demonstrate a “stiff” knee and hip approach to dynamic loading of the limb. Often the region “feels better” once “warmed up” but then hurts again later in the work out and at rest. The involved region will likely be tender but will not show signs of swelling (effusion) as the infrapatellar tendon is external to the knee articulation proper, making accumulation of inflammatory fluids unlikely. Athletes typically complain “stiffness” and pain after sitting for a time (i.e. long car rides) or on stairs, particularly descending.
Management of “Jumper`s Knee” follows typical strategies such as limiting exposure to offending training activities like bounding, and substituting more upper extremity gym work and double poling on snow or rollers. Cycling typically is tolerated well minus hard intervals. Jogging and hiking rarely go well. Swimming and “deep water running” utilizing a floatation device are useful training replacements.
Over the counter anti-inflammatory medicines can help modulate pain in the early stages of involvement, but there is debate regarding suppression of the bodies inflammatory/healing response via their use. Talk to your physician as appropriate. The same goes for icing (refer to Nordic Solutions, August 2019). Both interventions may allow the athlete to progress through a rehab program without interruption, and therefore have relative value. Physical therapy interventions such as electrical modalities, cold laser, gentle cross massage, and taping/strapping technique (to name a few) have beneficial effects. Efficacy of aggressive soft tissue work with or without “tools” is largely anecdotal and may induce further injury to the collagen matrix, already structurally compromised (de Vos et al. Br J Sports Med 2014).
Infrapatellar bands or straps, in the absence of IT Band Syndrome as a comorbidity, are typically helpful for load dispersion and are readily available commercially. They should be used sparingly to avoid blood flow compromise to the tendon.
Early stages of rehabilitation promote normalcy in the tendon from a vascular, neural and tissue matrix standpoint. Subsequent stages focus on “durability” and load tolerance. Exercise mode, dosage and attention to pain responses, are all vital to the progression. Skipping steps usually compromises the outcome, at least in the short term.
The abductors, extensors and external rotators of the hips require activation through band or weight resistive exercise as inhibitory weakness in these areas may lead to preloading of the infrapatellar region during limb flexion (via extremity adduction and internal rotation). Non weight-bearing (NWB) exercises should be selected in the early stages of rehab to avoid adverse infrapatellar loading.
Mechanical inputs from the ground up, in the form of foot pronation and obligatory tibial rotation, can also contribute to tendon loading. Calf flexibility and the use of orthotics are typically helpful.
Match your shoe and foot type! (a prior Nordic Solutions post)
Limb length asymmetry, with the involved side usually being long, can have deleterious inputs. Leg length differences are common. In an athlete, I typically correct anything over 3mm.
Isolated exercise for the quadriceps mechanism is the cornerstone of early rehab. Light, NWB/Open Kinetic Chain (OKC) sustained isometric contractions up to 90 seconds have been shown to stimulate favorable remodeling processes in tendon tissue. They also reverse motor cortex inhibition to the “injured” quad and can provide analgesia for up to 45 min post exercise (Cook JL et al. Br J Sports Med 2014 and Rio E et al. Br J Sports Med 2015). Repetitions range from 4 to 6 and may be completed daily as long as any post exercise pain elevation resolves within 12 hours of onset. Efforts should be between 25 and 50% of maximum and any induced pain during the effort should be no greater than 2 levels above resting status using a 0-10 pain analog. For example, if you have 2/10pain at rest and this rises to 4/10 with effort, you may proceed as long as your pain regresses back to 2/10 or less within 12 hours. Resistance sources can include ankle cuff weights, leg extension machines or resistive bands. This approach continues for approximately one week along with the afore mentioned hip work.
Recall that tendons are typically irritated via excessive tensile loading and/or compression. In the case of the infrapatellar tendon, this translates to firing the quad when the knee is in deep flexion (stretch pre-loading) or when the knee is in full extension/straight (tendon compression as it seats into the intercondylar groove of the femur). Neither of these postures should be used during the initial quadriceps loading phase. The preferred posture of the knee for early loading is between 30 and 60 degrees. This avoids potential pathomechanical inputs described above.
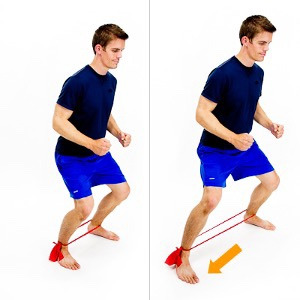
Closed kinetic chain (CKC ) exercises are introduced after the OKC phase if the athlete is improving. They are also initiated isometrically using body weight plus some form of external resistance. Placing exercise bands around the knees “cues” the athlete to activate the gluteal region and limit preloading of the infrapatellar zone. The same parameters are followed for CKC as the OKC work.
Lateral step and isometric ~45 degree knee holds below.
Eccentric loading is often utilized in the later stages of tendinopathy management, but there is limited high quality data to support this as a sole approach to loading (Malliaras P et al. Achilles and patellar tendinopathy loading programs: a systematic review comparing clinical outcomes and identifying potential mechanisms for effectiveness. Sports Med;43 , 2013) .
What is likely more important is the speed at which the tendon mechanism is loaded. Kongsgaard et al (Scand J Med Sci Sports,2009) proposed that Heavy Slow Resistance (HSR), whether delivered concentrically or eccentrically was the key to stimulate “durability” changes within the tendon. Three to 4 sets of 15 rep max (RM) efforts were advanced to sets of 6 RM loads between 10 and 60 degrees of knee motion. Squats, leg press, knee extensions and split squats were suggested by the investigators.
Whether eccentric emphasis or con/eccen traditional modes are utilized, the key points are;
-slow contractile speed, i.e. 6-8 seconds to complete the motion
-start with moderate weight and progress to 6 RM loads
-start bilaterally and progress to unilateral work as tolerated
-use the same pain threshold (analog 0-10) parameters as in the isometric phase
-stay away from 70+ degrees of flexion and full extension of the knee
This process should continue until the athlete has no pain elevation during or after the session. It may take weeks based on how chronic or recurrent the problem is. The afore mentioned hip and cardio training of course continues through this phase. Balance drills should be added. I suggest keeping one weekly OKC isometric session with progressive loading, in the program indefinitely.
The final phase of rehab prior to a full return to snow is the functional “rapid load, storage and release” mode of exercise, or plyometric progression. Dosage/repetition, load/depth and speed of the efforts are very important to monitor. Any signs of intolerance should terminate the activity and the athlete should revert to the prior phase of rehab and continue from there.
This site has an amazing selection of plyometric box jumping, bounding, and band resistance options for the athlete to experiment with.
So, whether Jumper`s Knee is the result of a long and hard race season, or preparatory errors in the pre- season, early recognition, adaption and implementation of a structured rehab program will likely arrest the symptoms, reverse the aberrant physiologic process and allow for a return to unhindered skiing.
Next, Patella Femoral Dysfunction.